

AARP Hearing Center



























































The Senate Health Reform Bill Would Slash Medicaid Severely
By Susan Reinhard, Jean Accius, Lynda Flowers, and Ari Houser, June 23, 2017 08:32 PM

The Better Care Reconciliation Act (BCRA) now under consideration in the Senate would drastically alter the Medicaid program. The proposed Senate bill would change the way the federal government currently funds Medicaid by limiting federal funding and shifting cost over time to both states and Medicaid enrollees. BCRA would subject older adults, adults with disabilities, expansion adults, and non-disabled children under age 19 to mandatory per enrollee caps beginning in 2020. State Medicaid programs would have the option to choose between block grants and per enrollee caps for non-elderly non-disabled non-expansion adults.
The Senate bill would start out using the medical care component of the Consumer Price Index (M-CPI)—a measure of the average out-of-pocket cost of medical care services used by an average consumer—as the growth rate for per enrollee caps. However, beginning in 2025, it would slash the growth rate to the Consumer Price Index for all urban consumers (CPI-U)—a measure of general inflation that examines out-of-pocket household spending on goods and services used for everyday living. CPI-U does not tie closely to medical costs and will not reflect population growth or the impact of aging. To be clear, none of the proposed growth factors—M-CPI, M-CPI+1, and CPI-U— keep pace with the growth in Medicaid spending.
Although studies have examined the impact of Medicaid spending cuts in the House-passed healthcare bill over a 10 year period (e.g. [ CBO] [ CMS] [ Urban Institute]) we know of none that examine the impacts over a longer time horizon. To fill this gap, the AARP Public Policy Institute has developed a model that looks out an additional decade to capture impacts on Medicaid spending between 2027 and 2036.
By dramatically reducing the per capita cap growth factor beginning in 2025, we project that the Senate bill would cut between $2.0 and $3.8 trillion from total (federal and state) Medicaid spending over the 20-year period between 2017 and 2036 for the four non-expansion Medicaid enrollment groups: older adults, adults with disabilities, children, and non-expansion adults (children with disabilities are excluded because BCRA does not subject them to capped funding). A cut of this magnitude threatens the viability of the program in unprecedented ways and will increase the number of people who no longer have access to essential healthcare services and critical supports. The projections do not include the proposed cuts to the adult expansion population, which would also be considerable.
Previous analysis by the AARP Public Policy Institute discusses why capping Medicaid is flawed and would leave states and the poorest and sickest Americans holding the bag for the shortfalls that will most certainly occur.
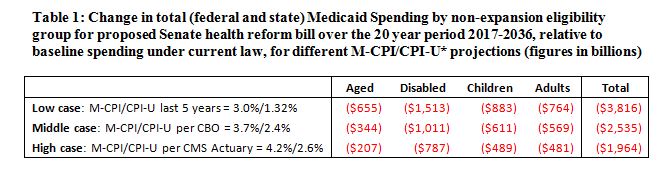
Table 1 shows the cumulative 20-year cuts to Medicaid by eligibility group under the Senate health reform bill for three growth rate projections. The bill would cap per enrollee cost growth using two measures of inflation (M-CPI and CPI-U), which are highly variable and uncertain, though well short of what is needed to maintain the integrity of the Medicaid program. It is difficult to plan for such uncertain growth rates, and reasonable projections are far apart.
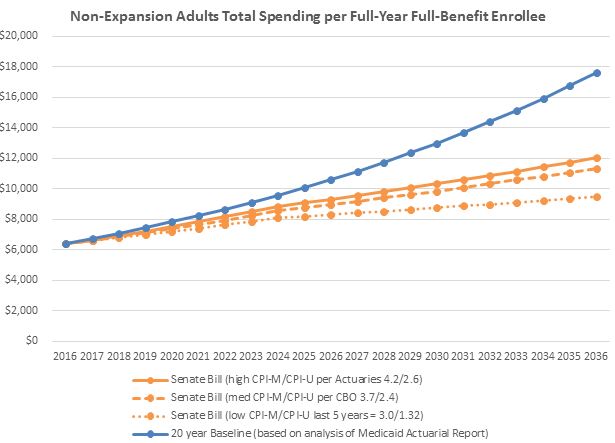
We present the high, middle, and low case for M-CPI/CPI-U growth rates based on the following:
- Low Case. Based on historical growth rates. Over the last five years (2012-2016), the M-CPI growth rate has averaged 3.0% per year, and the CPI-U growth rate has averaged 1.32% per year.
- Middle Case. Based on projections from the Congressional Budget Office. CBO projects M-CPI to grow by 3.7% per year, and CPI-U by 2.4% per year.
- High Case. Based on projections from 2016 CMS Medicaid Actuarial Report. From 2019 onward, this report projects M-CPI to grow by 4.2% per year, and CPI-U by 2.6% per year.
In short, the lower the cap growth rate, the more severe the Medicaid cuts will be.
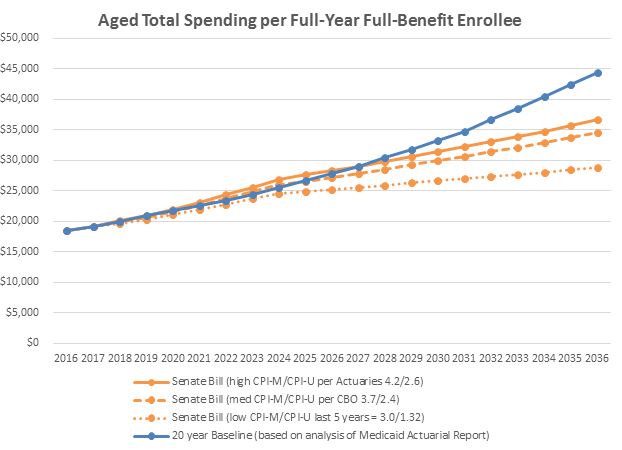
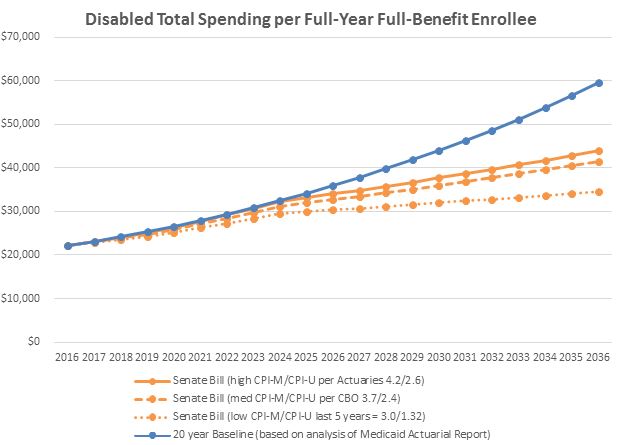
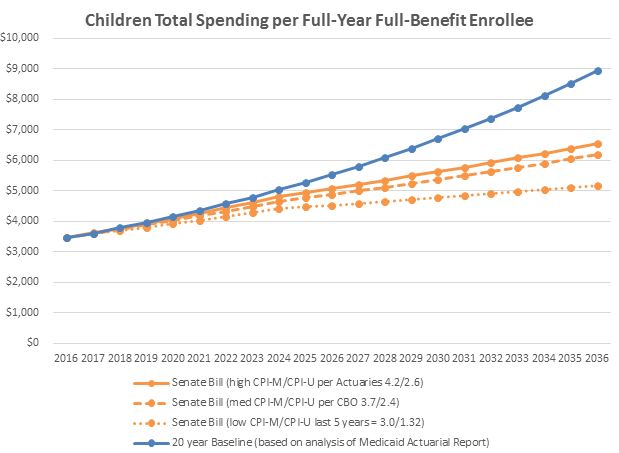
The charts below demonstrate that for any projection of the bill’s cap growth rates, BCRA will lead to significant funding shortfalls for older adults, adults with disabilities, and non-disabled low-income children and adults. The end result is that states and beneficiaries will be left with severe funding shortages, and states will be forced to cut eligibility, provider rates, or covered services—or very likely all three.
Dean, Olivia
Susan Reinhard is a senior vice president at AARP, directing its Public Policy Institute, the focal point for AARP’s public policy research and analysis. She also serves as the chief strategist for the Center to Champion Nursing in America, a resource center to ensure the nation has the nurses it needs. 

Jean Accius is vice president of livable communities and long-term services and supports for the AARP Public Policy Institute. He works on Medicaid and long-term care issues.

Lynda Flowers is a Senior Strategic Policy Adviser with the AARP Public Policy Institute, specializing in Medicaid issues, health disparities and public health.

Ari Houser is a Senior Methods Adviser at AARP Public Policy Institute. His work focuses on demographics, disability, family caregiving, and long-term services and supports (LTSS).
Search AARP Blogs
Recent Posts