

AARP Hearing Center



























































Proposed Change to Medicare Drug Price Negotiation Warrants Deeper Scrutiny
By Leigh Purvis, April 29, 2025 10:47 AM

The Inflation Reduction Act (IRA) of 2022 includes many provisions designed to address high prescription drug prices and related out-of-pocket costs. One of the most notable changes allows Medicare to negotiate the prices of certain high-cost prescription drugs, which is expected to save Medicare and taxpayers billions of dollars.
Medicare has already successfully negotiated lower prices for ten Part D drugs and another fifteen Part D drugs will have their prices negotiated by the end of 2025. The prices negotiated in the first and second rounds of Medicare drug price negotiation will become available in 2026 and 2027, respectively, and additional groups of drugs will be selected and negotiated every year. Medicare Part B drugs will become eligible for negotiation starting in 2026.
Medicare drug price negotiation is strongly supported by people across the political spectrum. However, even though the first negotiated prices have yet to become available, there are already efforts to extend the already considerable amount of time that must elapse before drugs become eligible for negotiation, which could greatly reduce savings from this important new program.
Negotiation selection process differs by drug type
Traditional (or non-biologic) drugs, which are typically taken orally, cannot be selected for Medicare drug price negotiation until it has been at least 7 years since they were approved by the US Food & Drug Administration (FDA). In contrast, biologic drugs, which are typically injected or infused, cannot be selected unless it has been at least 11 years since they were approved. Medicare-negotiated drug prices take effect two years after the drugs are selected, meaning they do not become available until the drug has been FDA-approved for at least 9 or 13 years, respectively.
Some argue that this inconsistency has created a so-called “pill penalty” that discourages investment in non-biologic drugs, and that all drugs should have at least 13 years on the market before a Medicare-negotiated price could become available. However, independent researchers have not found any meaningful evidence that the “pill penalty” is disincentivizing research and development for non-biologic drugs, and mergers and acquisitions have actually increased among companies developing non-biologic drugs, indicating continued interest in developing such products.
Equally important, this criticism overlooks that biologic drugs have always had significant market advantages that should make them more financially attractive to drug companies, yet the non-biologic market has continued to thrive.
Biologic drugs have longstanding advantages over non-biologic drugs
Non-biologic drugs fall under the purview of the Federal Food, Drug, and Cosmetic Act, which has included a streamlined process to approve generic versions of brand name drugs since Congress passed what is commonly known as the Hatch-Waxman Act in 1984. In contrast, most biologic drugs are regulated under the Public Health Service Act, which did not have an equivalent approval pathway until the Biologics Price Competition and Innovation Act (BPCIA) became law in 2010. This delay effectively resulted in a nearly 30-year long period where only non-biologic drugs faced the possibility of direct competition.
Further, the BPCIA did not fully level the playing field between biologic and non-biologic drugs. FDA typically grants exclusivity periods to newly approved prescription drugs that effectively prevent generic or biosimilar competitors from entering the market. Under Hatch-Waxman, new non-biologic drugs typically have a market exclusivity period of 5 years. In contrast, under BPCIA, new biologic drugs have a market exclusivity period of 12 years, nearly two and a half times longer than what is granted to non-biologic drugs.
In addition, BPCIA has not resulted in biosimilar competition that is comparable to generic competition under Hatch-Waxman. Most non-biologic drugs face generic competition as soon as their patents expire. In contrast, only 14 biologic drugs currently have biosimilar competitors in the US market, and only 10 percent of the nearly 120 biologic drugs whose monopoly periods are expected to end over the next decade have biosimilar competitors in development. While there are a wide range of reasons that the biosimilar market is struggling, the net effect is that biologic drugs are at significantly lower risk of facing direct competition from biosimilar drugs once their monopoly period ends.
Yet another advantage for biologic drugs is their price. Even though biologic and non-biologic drugs have comparable development times and costs, biologic drugs are often significantly more expensive, with prices that can reach as high as $500,000 per year. Such high prices can generate correspondingly high revenues even with relatively low utilization, making biologics an attractive prospect for profit-seeking drug companies.
Non-biologic drug market continues to thrive
Despite considerable and longstanding advantages that should make biologic drugs more financially attractive to drug companies, the pharmaceutical market is not showing signs that it has meaningfully shifted in that direction. While the overall number of new FDA-approved drugs fluctuates each year, the share of newly approved brand name drugs that are biologics has averaged around 30 percent for the past decade.
Share of new drug approvals that are non-biologics vs biologics, 2015-2024
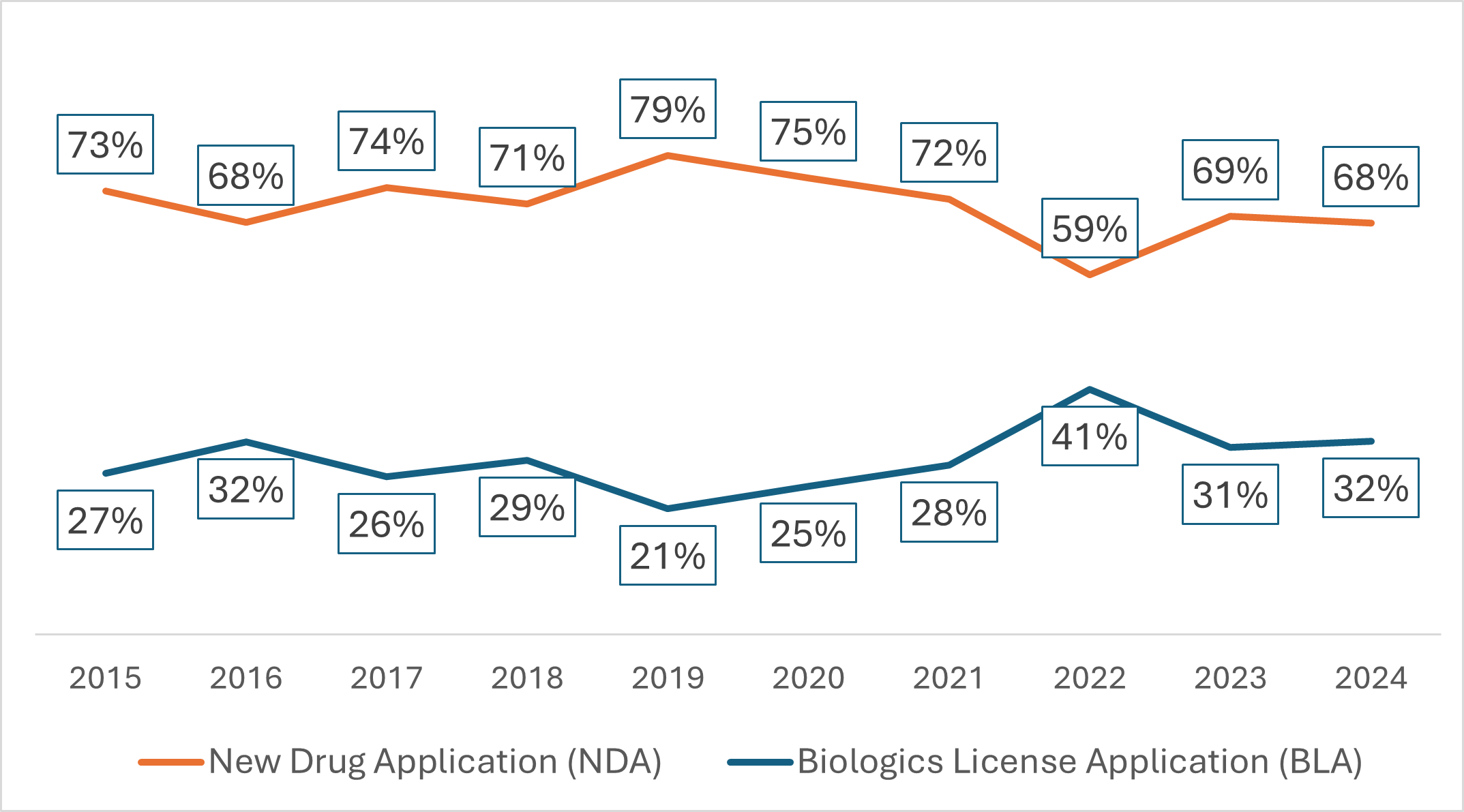
Source: AARP Public Policy Institute analysis of US Food & Drug Administration, “Compilation of CDER New Molecular Entity (NME) Drug and New Biologic Approvals,” https://www.fda.gov/drugs/drug-approvals-and-databases/compilation-cder-new-molecular-entity-nme-drug-and-new-biologic-approvals.
Note: Products were grouped under their original FDA approval method.
This relative stability suggests that factors other than financial considerations are effectively limiting how many biologics reach the market. For example, non-biologic drugs are easier to manufacture and distribute, preferred by patients over products that are injected or infused, and better suited to treat certain chronic conditions, none of which would be mitigated by changes to Medicare drug price negotiation.
Changes to Medicare drug price negotiation must be evidence-based
Thus far, Medicare drug price negotiation appears to be working as intended. The first 25 drugs selected for negotiation are used by millions of Medicare Part D enrollees and account for nearly $100 billion in total Part D spending. The expected savings are also considerable: the Centers for Medicare & Medicaid Services estimated that, had the first 10 negotiated drug prices been in effect in 2023, they would have lowered net Part D spending by 22 percent and created significant savings for people in Medicare Part D plans.
The savings from Medicare drug price negotiation also help offset other changes in the 2022 prescription drug law that reduce Part D enrollee costs, including a new annual out-of-pocket spending limit for people in Part D plans. Without Medicare-negotiated drug prices to help reduce overall spending, the cost of this improved coverage would result in significantly higher Part D plan premiums that could eventually become unaffordable.
Despite the importance of these improvements, critics of Medicare drug price negotiation want to change the program before the first negotiated price goes into effect, arguing that biologic drugs’ longer exemption from being selected for negotiation will discourage the development of non-biologic drugs. However, there is currently no independent research that supports this conclusion.
Moreover, it is unclear how Medicare drug price negotiation—which despite saving Medicare nearly $100 billion will cost drug companies less than 1 percent of their revenues over 10 years—will have more influence on drug company decision making than the multiple market advantages that have been available to biologic drugs since FDA first started approving them in 1982. If anything, these factors strongly suggest that those concerned about disparities between non-biologic and biologic drugs should support reducing the negotiation exemption period for biologic drugs instead.
Allowing Medicare to negotiate drug prices is a historic change that will provide billions in savings for the Medicare program, its beneficiaries, and American taxpayers. Any proposals to modify the negotiation process must be guided by conclusive evidence and appropriately targeted to ensure that drug company profits are not prioritized over much-needed savings for Medicare and its beneficiaries.

Search AARP Blogs
Recent Posts