

AARP Hearing Center



























































COVID-19 Hitting Blacks and Hispanics Hardest: Let’s Talk Solutions
By Lynda Flowers, Claire Noel-Miller, Olivia Dean, June 22, 2020 07:27 AM

In the face of the outbreak, AARP is providing information and resources to help older people and those caring for them protect themselves from the virus and prevent it spreading to others. You can find AARP's coronavirus resources at www.aarp.org/coronavirus.
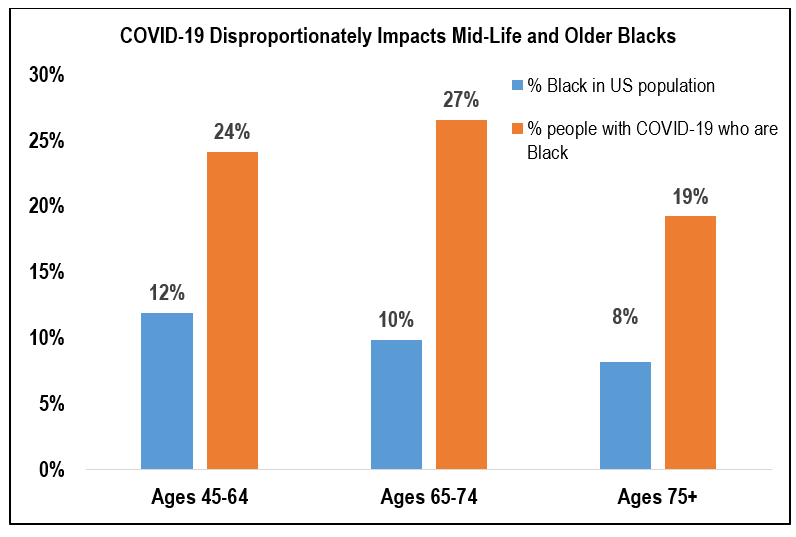
By now, you have likely heard the alarming news: the COVID-19 pandemic is hitting mid-life and older Blacks and Hispanics especially hard. While 12 percent of Americans ages 45 to 64 are Black, they represent a disproportionate 24 percent of COVID-19 cases in this age group. The discrepancy is similarly striking for older Black Americans (see figure). Emerging data indicate similar trends among Hispanics.
One important reason for the coronavirus’ disproportionate impact on midlife and older Blacks and Hispanics is a higher prevalence of underlying health conditions—like obesity, diabetes and high blood pressure—that increase the risk of COVID-19-related illness and death. These health disparities are the result of a longstanding history of racism that drives structural inequality and provider bias in health care decision making.
In a previous blog, we called for actionable solutions to reduce the disproportionate impact of COVID-19 on Blacks and Hispanics, starting with the urgent need to improve the collection of COVID-19-related data by race and ethnicity across all health and long-term care settings. Here are three other areas where immediate action will help push us forward:
1. Access to health coverage for midlife adults
The Affordable Care Act’s Medicaid and Marketplace coverage expansions improved access to coverage for millions of Black and Hispanic Americans. Those gaining coverage had an unprecedented opportunity to access preventive care and treatment for chronic illnesses before the current pandemic hit the United States. This is important for two reasons. First, properly managing health conditions has the potential to lower the risk of serious illness from COVID-19. People who lack access to coverage are less likely to have their chronic health conditions managed. In addition, those without health insurance may be less likely to seek coronavirus testing and more likely to avoid care if they get sick.
While Medicaid coverage expansions narrowed racial and ethnic disparities in access to coverage, 14 states have still not expanded their programs. Expanding the Medicaid program in the remaining states would provide critical access to care for over a million low-income midlife adults, including many midlife Blacks and Hispanics.
2. Food security
Access to healthy foods is critical to mid-life and older adults managing chronic health conditions, maintaining a healthy weight and building a strong immune system—all of which can help them better fight COVID-19. Even before the current crisis, food insecurity disproportionately impacted older Black and Hispanics, and the pandemic and associated economic crisis have only made it harder for many to access the food they need. Federal policymakers should shore up home-delivered meals and ensure those previously receiving meals in group settings have safe, alternative ways of getting food. They should also expand SNAP (formerly food stamp) benefits and allow for program flexibilities during this crisis.
3. Bias-free health care
Racial bias in health care is not new. Ample evidence shows that unconscious attitudes and stereotypes associated with patients’ race or ethnicity can influence health care providers’ decision making. Such implicit bias has been linked to worse health outcomes among older Black and Hispanic adults. During the current crisis, racial bias among health providers can have serious consequences. For example, a recent analysis suggests that physicians may be less likely to refer Blacks for testing when they come to a hospital with possible symptoms of COVID-19. This kind of bias could be contributing to the disproportionately high COVID-19 mortality rates among Blacks and Hispanics.
In the midst of the current pandemic, clinicians have a unique opportunity to address the problem of bias in health care. Rapidly increasing ongoing bias awareness training and education could help clinicians on the front lines of COVID-19 care actively acknowledge and manage their biases when seeing patients and making testing and treatment decisions. Another idea is for health care facilities to post reminders that ask care providers to “check your bias at the door” and presenting bias-related content in the context of specific workplace scenarios. Finally, health care administrators can take into account any impacts on vulnerable populations when allocating health care resources, to ensure that funding priorities reduce disparities.
Three Steps Closer But Much More to Do
Protecting vulnerable communities hit hard by the coronavirus pandemic requires swift action. Ensuring that mid-life and older Black and Hispanic adults have access to health care coverage, adequate nutrition and bias-free health care can help protect them from the worst of the pandemic’s impact.
Longer term, policy makers and others must do much more to address the root causes of health disparities, including those related to COVID-19. To do so, they must understand and be willing to craft solutions that address the structural inequities that drive these disparities—such as the stressors associated with institutional racism, access to adequate and affordable housing, safe neighborhoods, and good paying jobs, to name just a few. Racial and ethnic disparities in health outcomes are rooted in centuries of racism and structural inequality, and eliminating them will require bold action from all parts of society.



Search AARP Blogs
Recent Posts